There are more than 700,000 autistic people in the UK. Many autistic children and young adults experience a delayed diagnosis, which can have a significant negative impact on their mental health.
We hear from Freddy Henderson (she/her) about her experiences being diagnosed with Autism Spectrum Disorder (ASD) and her reflections on what mental health services can do to care for autistic people in a more effective and person-centred way.
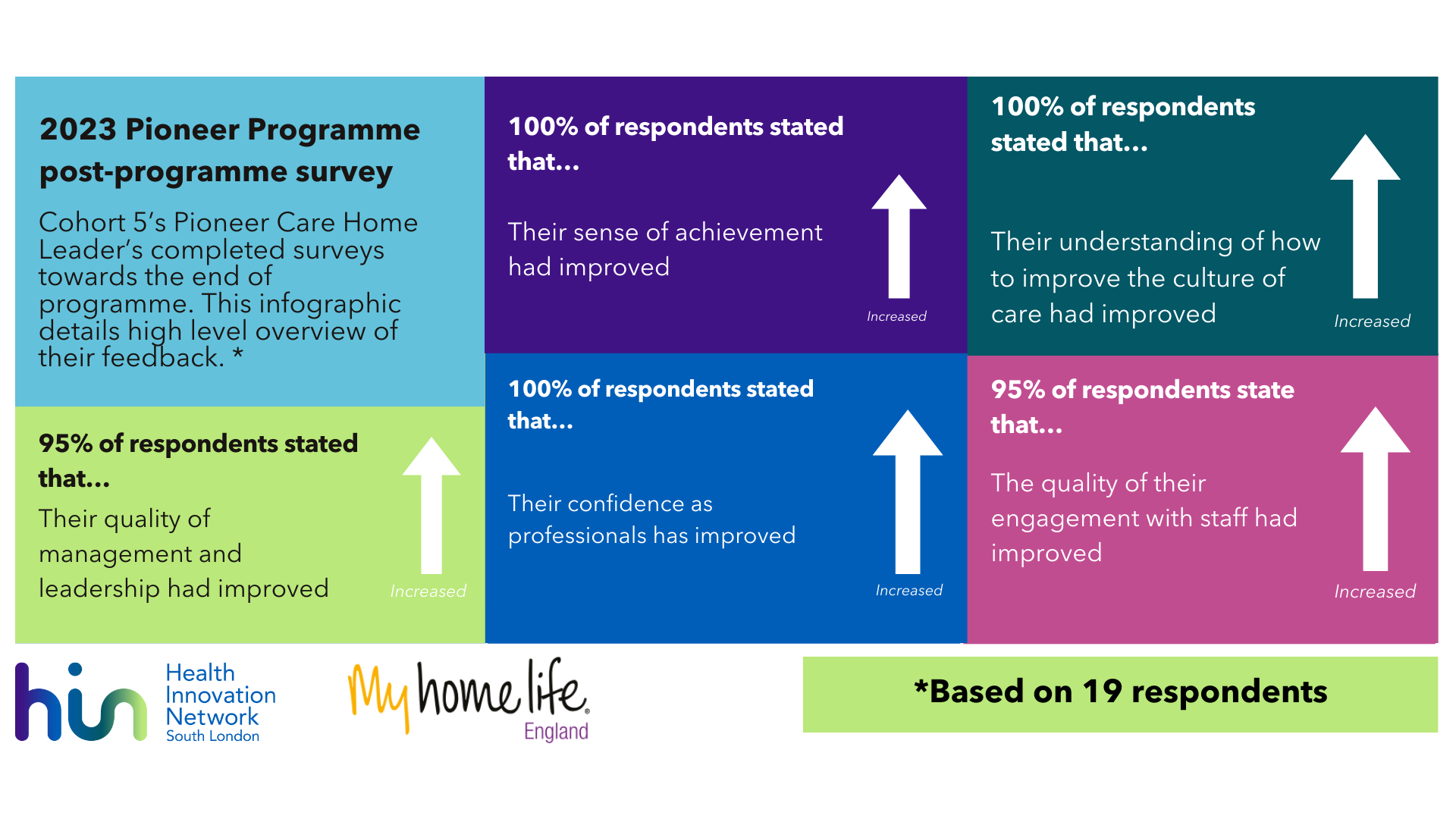
Freddy also discusses how innovations such as Tellmi can provide valuable access to safe, anonymous peer support for autistic children and young people, who may often prefer to use digital channels. Tellmi is an innovative digital peer support app which is commissioned by the NHS and has been used by more than 80,000 young people to discuss their mental health.
Please note that this article contains some mentions of self-harm, suicide and eating disorders which some readers may find upsetting.
I have 2 disabilities, Functional Neurological Disorder (FND) and ASD, although the latter is what I am going to be talking about today. I was diagnosed with autism six years ago, at age 17. That diagnosis came about after I was referred to the integrated neurodevelopmental team by Child & Adolescent Mental Health Services (CAMHS) as they suspected I was autistic. I had originally been referred to CAMHS when I was 15 by my school, as I was suffering a lot with my mental health and was grappling with self harm, depression and anxiety. I later developed anorexia and so was also under Child & Adolescent Eating Disorders Services (CAEDS) for about three months until I turned 18. Later at university I accessed NHS services in conjunction with the university resources to help me balance my mental health needs and medication for it.
I want to highlight that my ASD was not the direct reason I was using these services, but rather that I needed these services because the effects of my late diagnosis had become so catastrophic that it ‘broke’ my ability to cope with the world.
What I hope I can give an insight on in this blog is my own perspective what was helpful, what was not, and how I think services and treatment could be improved.
The bad
Let’s start with the worst of my experiences to get them out of the way.
My first therapist at CAMHS was terrible. They made me feel belittled and patronised, and their complete failure to understand my attempts at communicating what was going on meant that my health got actively worse.
I was very quiet and reserved in sessions and had flashes of anger when my therapist tried to make suggestions; I felt attacked and as though they were accusing me of not trying hard enough. I never shouted or expressed that anger outwardly, but it meant I was defensive and ardently against sharing information that I deemed to be too personal.
At the start of one session my therapist walked in and put a colouring book and pencils on the table and told me to colour. After a few minutes, I asked if we were going to talk. They replied with “well if you’re not willing to talk to me, why should I talk to you?”.
A couple of days later I was held overnight in hospital after a bad self-harm incident, which led to meeting my next therapist.
The next therapist made me feel much better. They were kind and patient with me and gave me practical help with how to formulate sentences expressing my thoughts and feelings. They would ask direct questions rather than open-ended ones, something that helped immensely.
We’ll come back to them later, but first let’s quickly talk about another bad experience.
It is now widely recognised that eating disorders are rife within the autistic community (especially young people) and I was no exception. What started as a desire to get “in shape” quickly morphed into a monster beyond my control.
I won’t describe any of my thoughts, actions or physical consequences as eating disorders are notoriously competitive and I don’t want to trigger other people who might be vulnerable themselves. The only part relevant to this story is that I was very unwell.
I was only in CAEDS treatment for about three months just before I turned 18, and so was transferred to the adult services where I promptly discharged myself after the therapist there criticised me for not making eye-contact with them.
Any readers with a vague understanding of autism may see the issue here. Eye contact is often difficult for autistic people and I don’t look at people’s eyes at any time, let alone when I’m feeling vulnerable. By this time, I had my diagnosis and the sheer disregard for my condition and the traits it presents as meant I rejected all additional treatment for my anorexia.
I am very pleased to say that I no longer have anorexia as I put in a lot of hard work and, with the help of some borrowed ideas from the fat acceptance movement, managed to overhaul the disease that controlled me for 3 years.
The (mostly) good
Now, onto the good experiences!
My second primary therapist was the person who helped me get an autism diagnosis, which turned out to be one of the biggest turning points in my mental health journey.
Up until that point I genuinely believed that I was fundamentally flawed as a human being and there was something intrinsically wrong with me. I considered myself nothing short of a complete waste of space and that my life would forever be spent in pursuit of a goal I would never achieve.
Getting my diagnosis put a stop to most of these thoughts, although it remains difficult to completely dismiss ideas you have held for the majority of your life.
It helped me come to terms with my differences and understand that I was not ineffectual as a human being, but rather I just operate a bit differently.
I was able to recognise my strengths for what they were, rather than consider them some minor penance for my otherwise catastrophic flaws. The diagnosis helped me to separate my brain from my mental health disorders. It helped me understand why I thought the way I thought and act the way I act.
It also helped explain why so much of the therapy I had had had been ineffective. Of course the CBT for panic attacks hadn’t worked; I wasn’t having panic attacks, I was having meltdowns.
Another type of support that helped hugely was when I met other autistic people.
At my university there was an autism support group. Granted, it was run by non-autistic staff members and in my third year it took such a drastic turn for the worse that I left after arguments with said staff, but still. I met a couple of good friends there who I miss dearly as we are no longer in the same city.
Meeting other people like me was amazing. We were able to connect on a level I hadn’t experienced before as we had an innate understanding of each other. That is not to say that my friendships with autistic people are inherently better than those with non-autistic people – they are just different.
Of course, autistic people are not a monolith and so there were some people there who I really disliked. Regardless of the ups and downs – being able to talk about our shared experiences was such a relief.
During my second year at university, the pandemic hit.
Covid-19 impacted every aspect of our lives, including the support services I was in. I got removed from the NHS community mental health service and the university wellbeing service as they wanted to free up capacity for people struggling to adjust to life in such a different world. The irony was not lost on me.
The ASD group was also moved online and let me tell you, trying to do a jigsaw puzzle over zoom presents some complications. I think it’s fair to say that aided in the breakdown of the group dynamic and made it quite difficult for the members who weren’t very confident to get to know the group.
We ended up doing activities such as a name-this-vegetable quiz, organised by one of the staff members. This quiz was later referenced when the whole group was arguing with the mentors that they were treating us like children.
The difference between in person support and digital support was stark. No one was ready for the pandemic and as everyone struggled to adjust, those accessing support services just plain struggled.
However, there was a definite silver lining to the switch to digital content and support: my university was online, which turned out to be an absolute godsend. By my second year I was still struggling with my mental health and processing a suicide attempt a year earlier. I had also started to develop what I now know is FND, although it would take roughly 4 years to get diagnosed.
In short, I was both physically and mentally really ill. Being able to do classes online was bizarre at first, but not having to expend energy getting to and from class and dealing with the sensory nightmare of being in public was amazing.
Lots of the pressure I had felt, both economically struggling at work and socially struggling on nights out, had been lifted. People found ways to socialise online, and jobs offered flexible working where possible. It hugely helped me.
The future
That is why going forward I am such a proponent of a hybrid approach to pretty much anything that can be hybridised. Whether it’s flexible office hours or the option of having therapy online, giving people the option to choose what suits them best hugely helped me and so many of my autistic and otherwise neurodivergent friends.
I still like going out with my friends, and having workplace banter is fun, but having seen the real benefits that digital services offer makes me very reluctant to go back to how things were.
And this is a key concept that I want to convey: when the world changed it was because it had to, but the effect was more surprising than anyone anticipated. All manner of people benefitted in unforeseen ways and thus having an open, flexible approach to resources and services is, in my humble opinion, the way forward.
Peer support does not have to be in person. Digital channels can be just as useful as in-person, and possibly more so when you consider factors such as geographical isolation, physical disability or time restrictions. Apps like Tellmi allow users to connect with others like them. Just as meeting my autistic friends was hugely helpful, having access to other people who may be experiencing similar issues is hugely helpful.
I’ve had the chance recently to speak with and work alongside the creators of the Tellmi app, and it seems clear that a lot of the reason why their service works for autistic people is because they put an emphasis on listening to and learning from autistic people to make their app better. Having people involved in the day-to-day running and development of the app who are neurodiverse is undoubtedly a good thing.
Consulting, engaging and co-producing with diverse groups of people will help build better solutions that work for all people. Just as neurodiverse people should be consulted about improving services for neurodiverse people, changes which have the potential to affect any group should be decided with the involvement of people who are representative of that population.
An underlying cause of the lack of effectiveness for many of the treatments I experienced was that they did not account for my autism. Autism is a fundamental part of me – and something I am very proud of – yet I was being funnelled through services not designed for people like me. As such, is it not surprising that they did not help me, and in some cases caused me harm?
Any support for autistic people needs the input of autistic people. And any services that might support autistic people also need the input of autistic people. You can have the best intentions in the world and be the brightest person alive, but if you haven’t lived as an autistic person, you will never build services which truly support autistic people alone.
Almost all the solutions I have found that have got me to where I am now have been of my own creation.
And where I am now is pretty darn great. I am happy, I am optimistic, and I am enjoying my life – which is much more than I could say when I was 15.
You might look at me, in my wheelchair with my headphones on and sunglasses blocking out external stimuli and think my existence is something which requires improvement. But I am at my best. Imposing one’s own ideas of how someone else should live is an issue for the ages, and that is precisely why it is imperative that we remove assumption and prejudice from the equation when we are trying to make services better for people.
I mostly don’t read work on autism by non-autistic authors. It is often derogatory, wrong or just plain offensive and I have no time for it.
My autism is a condition of which I take pride in and use to my advantage. I don’t have to be a genius like Einstein or a world changing advocate like Greta Thunberg in order to deserve the right to live as my authentic self.
I have no interest in support that hasn’t been developed by someone like me because it will be inherently steeped in presumptions and expectations that I don’t ascribe to. I will only ever be happy when I accept that I am not fundamentally flawed because of my condition and work alongside it to shape my life in the best way for me.
Interested in how digital technology can be used for mental health?
Speak to our expert team about how digital technology can be used to help mental health and wellbeing.
Get in touch